

INTRODUCTION
As in many countries over the past three decades, the mental health landscape in the United Kingdom has become increasingly complex, with wellbeing emerging as both a public health priority and a personal developmental concern. Government reports continue to highlight mental health and wellbeing as a key agenda (Department of Health, 2011a). Yet, national data suggest that traditional, treatment-focused responses have not sufficiently addressed rising levels of psychological distress. Between 1993 and 2014, self-reported mental health difficulties increased by one-fifth in England, with one in six adults now experiencing a mental health problem each week. In 2020–21 alone, the National Health Service (NHS) spent £14.3 billion on mental health services (Baker, 2021), with the broader cost of mental illness estimated at £105.2 billion per year (Department of Health, 2011b). These figures illustrate not only the scale of the challenge, but also the limitations of approaches that prioritize illness management over wellbeing promotion.
The COVID-19 pandemic significantly intensified these challenges. The Office for National Statistics (2021) reported that rates of moderate to severe depressive symptoms nearly doubled among adults, with stressors such as economic instability, social isolation, and health-related fears compounding psychological distress (Pierce et al., 2020). Service disruptions and digital exclusion during the COVID-19 pandemic disproportionately affected vulnerable groups, including people with pre-existing mental-health difficulties, ethnic minorities, and those with lower socioeconomic resources, thereby widening existing inequalities (Spanakis et al., 2021). While restrictions have lifted, longitudinal research indicates that elevated mental health needs are likely to persist (Fancourt et al., 2021). Recent data also show concerning increases in mental health difficulties among children and adolescents (Royal College of Psychiatrists, 2023), and increasing economic costs, estimated at £300 billion annually in England alone (Centre for Mental Health, 2024). Suicide rates have reached their highest levels in 25 years (ONS, 2021), and workplace stress and burnout continue to escalate (MHFA England, 2024).
However, as coaching and positive psychology have repeatedly emphasized, the absence of illness is not equivalent to the presence of wellbeing (Keyes, 2002; Seligman, 2011). A growing body of research highlights that wellbeing is multidimensional, involving emotional, psychological, and social components, and can be cultivated even in the context of adversity. Positive psychology and coaching psychology offer a strengths-based, developmental lens through which to understand and support adult wellbeing. Rather than focusing solely on symptom reduction, positive psychology coaching can highlight psychological resources such as self-efficacy, identity coherence, emotional regulation, meaning, and post-traumatic growth (Joseph & Linley, 2005), promoting flourishing and resilience, particularly in adulthood.
Mental health research tends to prioritize youth or clinical populations, leaving the wellbeing trajectories of adults over the age of 25 underexplored. Yet, adult identity development is a dynamic process shaped by significant life events. Research has shown that traumatic or highly impactful experiences, especially those perceived as central to a person’s self-concept, can have profoundly negative effects on psychological functioning (Berntsen & Rubin, 2006; Rubin et al., 2008). These central events may influence identity narratives, emotional processing and ultimately wellbeing. Shame, a self-conscious emotion strongly tied to identity, has been identified as a key predictor of psychological distress and lower wellbeing. Yet its interaction with identity processes in non-clinical adult populations remains less well-researched.
Given the rising prevalence of psychological distress, the limitations of treatment-focused approaches, and the growing evidence base for strengths-oriented, psychologically informed coaching interventions, there is a clear need for research that deepens understanding of the factors that predict and moderate wellbeing.
This study is situated at the intersection of positive psychology, identity theory, shame, and coaching psychology. It explores how identity and shame relate to psychological wellbeing in adults over 25 in the UK, and whether the centrality of a significant event moderates this relationship. Importantly, this research addresses a gap in the literature by examining these relationships in a non-clinical adult population through a coaching psychology lens, rather than focusing solely on symptom reduction or clinical outcomes. By investigating how these factors interact to support or undermine wellbeing, the study seeks to offer novel insights that can inform strengths-based, coaching approaches to adult psychological wellbeing, supporting individuals and communities to move beyond survival towards flourishing.
LITERATURE REVIEW
Wellbeing
Wellbeing is a multi-dimensional construct, which makes it difficult to define, with researchers often focusing on dimensions of wellbeing rather than a specific definition (Dodge et al., 2012). It is important to note that it is much more complex than just the absence of mental illness (Ruggeri et al., 2020). The American Psychological Association (2018) defines wellbeing as “a state of happiness and contentment, with low levels of distress, overall good physical and mental health and outlook, or good quality of life”, whilst the World Health Organization (WHO, 2004) incorporates wellbeing in their definition of positive mental health, saying “a state of wellbeing in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to contribute to his or her community”.
Both definitions focus on the individual’s ability to experience happiness within themselves, whilst the WHO’s definition also encompasses an individual’s ability to embed themselves successfully at both the individual and population level within their community.
In 2011, Seligman introduced the PERMA model, which conceptualizes wellbeing through five domains: positive emotions, engagement, relationships, meaning, and accomplishment. This model brought the principles of positive psychology into applied settings and provided a language for individual and organizational flourishing. However, subsequent work has highlighted the importance of considering broader contextual and systemic influences on wellbeing, arguing that wellbeing frameworks should incorporate social, environmental, and institutional factors (Kern et al., 2020).
In response, Donaldson et al. (2021, 2022) proposed the PERMA+4 model, which incorporates four additional pillars: physical health, mindset, economic security, and environment. This extended model acknowledges that wellbeing is shaped not only by psychological constructs but also by external conditions and broader social determinants. As such, the PERMA+4 framework may be particularly relevant when examining wellbeing in adult populations who have experienced adversity or trauma, as it captures both internal psychological functioning and external realities that may enhance or constrain wellbeing outcomes. The model offers a practical, evidence-based understanding of wellbeing as a multifaceted construct shaped by both internal and external domains. Therefore, the present study adopts the PERMA+4 model (Donaldson et al., 2022) as a guiding framework.
Identity Formation
Erikson (1956) introduced the term consolidated identity as one construct of identity formation, referring to an individual’s ability to show/receive intimacy and to demonstrate morals and values over a continued period, and is seen as the essence of identity and positively correlated to wellbeing. Achieving a consolidated identity is linked to a positive sense of wellbeing, increased happiness, improved mental health, increased adaptability within the world and surroundings, the ability to form intimate relationships, and higher levels of self-confidence and self-esteem (Erikson, 1956).
If an individual’s identity and self-concept do not conform to their environment, thoughts, and feelings, this may be referred to as a stage of disturbed identity (Sharma & Chandiramani, 2021). An individual may be unable to commit to and find their role within society, lack a self-concept, and be unable to take on others’ thoughts, feelings, and emotions, as they are unaware of their own (Kaufman et al., 2014).
Individuals may even suffer from a lack of identity (Kaufman et al., 2014), characterized by feelings of emptiness, soullessness, and a lack of continuity in self-image. A lack of identity may involve sudden, dramatic shifts in an individual’s thoughts, feelings, appearance, plans, sexuality, values, and friends. While it was thought that most identity crises occur during adolescence and early adulthood (Erikson, 1956), researchers have since found that identity disturbances can occur in adulthood (Al-Owidha et al., 2009; Cramer, 2004).
Although the PERMA model has been extensively studied in relation to wellbeing (Al-Hendawi et al., 2024; Seligman, 2011), research examining the relationship between identity development, particularly identity consolidation or disturbance, and PERMA outcomes is limited. Similarly, the expanded PERMA+4 framework has received little attention in the context of identity processes. However, key constructs discussed in this study, such as meaning, purpose, engagement, and relational connection, map directly onto core PERMA domains, suggesting potential conceptual alignment. This highlights a gap in the literature and suggests that exploring the relationship between identity and wellbeing through a positive psychology coaching lens could provide valuable insights into factors that support adult flourishing.
A lack of consolidated identity can cause psychological distress (Kaufman et al., 2014). It is linked to several DSM-5 diagnoses, such as borderline personality disorder, bipolar, eating disorders, depression, schizophrenia, and substance abuse (Sharma & Chandiramani, 2021). This suggests that identity status is an important psychological construct for coaching practitioners to consider.
Côté (2018) suggests that identity has been overlooked in research related to wellbeing and mental health. This view is supported by Sharma and Chandiramani (2021), who found a significant relationship between identity status and wellbeing. From a coaching psychology perspective, identifying the factors that strengthen this relationship may provide valuable insights into how individuals can be supported in enhancing self-awareness, resilience, and meaning-making. Such exploration could also inform the development of evidence-based coaching interventions in trauma-informed contexts.
The Role of Shame
Conceptually, shame is a self-conscious emotion rooted in the perception of the self as defective or unworthy (Tangney & Dearing, 2002). It is a complex, intense, and multifaceted emotion in which an individual perceives themselves as judged by others and as inadequate (Dolezal & Lyons, 2017; Velotti et al., 2016). As research into shame has developed, several forms of shame have been identified, including internalized shame, transient shame, humiliation, chronic shame, toxic shame, and even healthy shame (Dolezal & Lyons, 2017). Unlike guilt, which focuses on actions (“I did something bad”), shame targets the self (“I am bad”), making it especially potent in contexts of trauma, identity disruption, and diminished wellbeing (Tangney & Dearing, 2002). Shame is associated with increased risk of depression, anxiety, social withdrawal, and lower self-esteem (S. Kim et al., 2011), making it a very relevant topic when researching adult wellbeing.
A biopsychosocial model was introduced by Gilbert (1998) to try to explain the complex nature of shame. This model focuses specifically on the importance of social positions and cultural views, linking them to an individual’s ability to be socially aware and to experience shame. Tangney & Dearing (2003) discussed a different perspective to try to explain shame, suggesting that shame is experienced when there is a conflict between an individual’s real self (ego) and their idealized image of who they want to be (ego-ideal), causing conflict within themselves and their own morals, which in turn links to identity. A newer theory that builds on this is the appraisal-based model of self-conscious emotions. This model suggests that an individual will evaluate a situation to determine whether it is essential to self-representation. If a situation is perceived as meaningful, an individual may turn to self-evaluation, which then, in turn, may lead to feelings of shame (Tracy and Robbins, 2004). As this study focuses on internalized shame, the appraisal-based model will be examined.
Although shame is now considered within many medical settings, the relationship between internalized shame in adult populations and wellbeing is still underexplored, with most research focusing on marginalized groups in relation to medical conditions, e.g. obesity (Duarte et al., 2017).
Shame, Trauma and Identity
In comparison to guilt, shame implicates the global self and can persist long after a precipitating event has passed. This is especially the case when the traumatic event is perceived as central to one’s life story (Robinaugh & McNally, 2011). In the aftermath of trauma, shame often becomes internalized, leading to chronic self-blame, emotional withdrawal, and disrupted self-concept (Gilbert & Irons, 2005). This may function as a mechanism through which the centrality of event enhances identity disturbance, thereby reducing wellbeing. Furthermore, the presence of shame may undermine the integration of difficult experiences into a coherent identity narrative, particularly when those experiences contradict ideal or expected self-states (Higgins, 1987). Exploring shame within this framework would not only address a gap in adult mental health research but could also offer insight into how persistent self-evaluative emotions can influence psychological recovery and flourishing after trauma.
This study focuses on internalized shame: an individual’s negative shame views of themselves (Gilbert, 2000). It is important to note that whilst an element of shame can be healthy and enable an individual to understand both their own and others’ boundaries, as well as helping them understand how their behavior may affect others (Rollins & Crandall, 2021), most feelings of shame are deep rooted in self-criticism and a negative view of oneself, detrimentally affecting an individual’s wellbeing (Yakeley, 2018).
Centrality of a Traumatic Event as a Moderator
Trauma is defined as a deeply distressing or disturbing experience that can significantly impact an individual’s mental, emotional, and social wellbeing (American Psychiatric Association, 2013). This is usually viewed in a negative light, and the centrality of an event (CES) refers to the extent to which they perceive the trauma as central to their life story (Wamser-Nanney et al., 2018). Negative CES views have been shown to positively correlate with depression, feelings of shame and identity questioning (Berntsen & Rubin, 2006), which in turn negatively affects an individual’s wellbeing (Kaufman et al., 2014).
The CES has been shown to be a moderator of post-traumatic stress disorder (PTSD), self-acceptance, purpose, and growth (George et al., 2016; Wamser-Nanney et al., 2018). These elements play key roles in identity formation and feelings of shame (Bakaitytė et al., 2022; Eze, 2022), highlighting the importance of understanding the moderating role CES plays in the relationship between these variables.
Trauma and Identity
Berntsen & Rubin (2006) found trauma can influence an individual’s life story and understanding of self, becoming a central component of an individual’s identity, and depending on their perception, potentially negatively affecting their wellbeing. This is supported by Merrill et al.'s (2015) findings that individuals who perceived events negatively were more likely to experience higher psychological distress and identity diffusion, suggesting that the impact of CES can strengthen the relationship between wellbeing and identity.
Trauma can also lead to post-traumatic growth, when an individual’s baseline wellbeing rises after a traumatic event (Jayawickreme, 2020; Park & Helgeson, 2006). A recent study by Popescu et al. (2025) found that narrative reframing interventions could reduce shame and cultivate hope in families who had experienced trauma. By reframing themselves as survivors as part of their identity, they were able to improve relationships within their family, turn trauma into meaning, and grow and survive, turning their suffering into positive change and improved wellbeing.
The Interplay Between Identity, Shame, and the Centrality of Experience in Adult Wellbeing
Emerging research in coaching and positive psychology suggests that adult wellbeing is influenced not only by emotional states or the absence of mental illness, but by the internal frameworks through which individuals make sense of past experiences. In particular, shame, identity, and the subjective centrality of adverse or formative events can act as interacting psychological mechanisms that shape wellbeing outcomes across the lifespan (McLean et al., 2019).
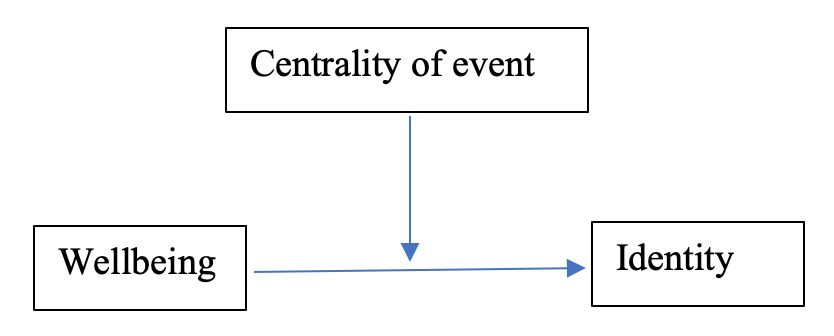
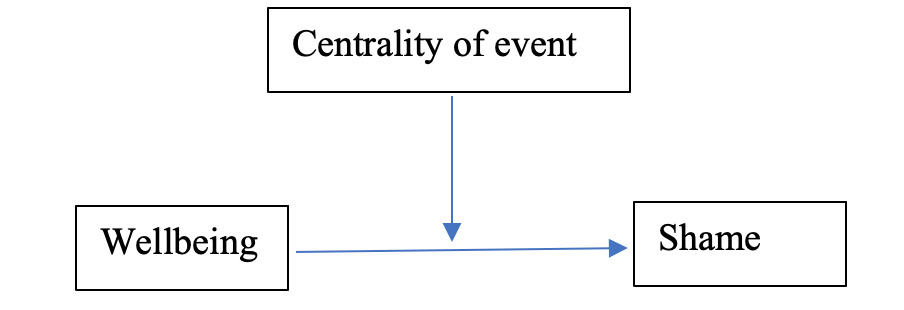
Crucially, this study investigates whether centrality of event (CES) acts as a moderator in the relationship between both shame and identity and the outcome variable of wellbeing. The CES assesses the degree to which a past event is seen as pivotal, identity-defining, or explanatory of one’s life narrative (Berntsen & Rubin, 2006). In this context, moderation analysis tests whether the strength of the relationship between identity or shame and wellbeing varies depending on the level of event centrality. In other words, it examines whether the psychological impact of shame or identity disturbance on wellbeing is stronger or weaker when the triggering event is perceived as more central to the individual’s life story. Specifically, the analysis tests whether the association between identity disturbance and wellbeing becomes stronger when individuals perceive a traumatic event as highly central to their life narrative. This is especially relevant for adult populations over 25, who may retrospectively re-evaluate prior life events as part of meaning-making and identity reformation processes.
By exploring these constructs together in a UK adult population over the age of 25. It also addresses a gap in the current literature by situating centrality of event as a potential amplifying mechanism, capable of shaping the emotional weight and psychological impact of shame and identity disruption.
Aims of the Study
This study aims to understand the interplay between identity disruption, shame, and wellbeing, and whether the perceived centrality of a past event strengthens these relationships. This integrative approach addresses gaps in adult mental health research and offers insights into the psychosocial mechanisms that can inform coaching interventions aimed at enhancing resilience, self-concept clarity, and overall flourishing.
It asks if:
-
Higher scores of wellbeing would result in fewer feelings of shame and identity exploration, and if higher scores of shame/identity would result in lower wellbeing.
-
Centrality of an experienced traumatic event moderates the relationship between wellbeing and identity by strengthening the relationship.
-
Centrality of an experienced traumatic event moderates the relationship between wellbeing and shame by strengthening the relationship.
METHOD
Design and Participants
The study is a cross-sectional study exploring the relationship between the independent variable wellbeing and the dependent variables of identity and shame. Additionally, it explores whether centrality of an experienced traumatic event is a moderator of the relationships.
Before recruitment, ethical approval for the study was obtained through Northumberland University. Participants were recruited through opportunity sampling by distributing an invitation to participate via the researchers’ existing social media networks. Participation was voluntary with no reward. Adults over the age of 25, residing in the UK, who had not been officially diagnosed with a DSM-5 dissociative identity disorder were eligible to participate in the study. This exclusion was to ensure that all participants had a cohesive, stable identity. In total seventy-six participants (15 men and 61 female) were recruited. No recruited participants were identified with dissociative identity disorders, including dissociative amnesia or depersonalization/derealization disorder, so no exclusions applied.
Scales Used
After agreeing to participate, participants completed the following questionnaires on Qualtrics.
Warwick-Edinburgh Mental Well-being Scale (WEMWBS)
The WEMWBS is a 14-item self-report scale which measures mental wellbeing, with a specific focus on positive elements of mental health. The 14 items are rated on a 1-5 Likert scale (1=None of the time, 5 = All of the time), and are positively worded, including questions such as: “I’ve been feeling useful” and “I’ve been feeling loved” (Tennant et al., 2007. WEMWBS demonstrates good content validity and excellent internal consistency with a Cronbach’s alpha score of α=0.95.
The Self -concept and Identity Measure (SCIM)
The SCIM is a 27-item, self-report measure of disturbed and healthy identity, which measures the subdomains of disturbed identity, consolidated identity, and lack of identity. Participants are asked 27 items on a Likert scale 1-7 (1=strongly disagree – 7 = strongly agree). Questions from each subdomain include: “I know what I believe” (consolidated identity), “I change a lot depending on the situation” (disturbed identity) and “I am broken” (lack of identity) (Kaufman et al., 2014). Within this study, the SCIM demonstrates good internal consistency with a Cronbach’s alpha score of α=0.65. For the purposes of the present analysis, an overall SCIM composite score was used rather than analyzing the three subdomains separately.
Guilt and Shame Proneness Scale (GASP)
The GASP scale is a 16-item self-report measure of an individual’s experiences of shame or guilt within different scenario-based questions, which includes four subscales: guilt negative behaviour evaluation (NBE), guilt repair (GR), shame negative self-evaluation (NSE) and shame withdraw (SW). Participants are asked to imagine if they would react to a scenario within the stated way using a Likert scale of 1-7 (1=Very Unlikely, 7 = Very Likely). While participants were asked all questions, only the shame NSE subscale was used, an example of a question from the NSE subsection includes: "You make a mistake at work and find out a coworker is blamed for the error. Later, your co-worker confronts you about your mistake. What is the likelihood that you would feel like a coward?" (Cohen et al., 2011) . The shame NSE subscale demonstrates good internal consistency Cronbach’s alpha score of α=0.74.
The Centrality of Event Scale (CES)
The CES scale is a 20-item scale that measures the extent to which a memory of a past traumatic event influences an individual’s personal identity and self-awareness, and the attribution of meaning to other life events. Participants are asked 20-items using a 1-5 Likert Scale (1=Totally Disagree, 5= Totally Agree). They are initially asked “Please think back upon the most stressful or traumatic event in your life and answer the following questions in an honest and sincere way” and then asked questions such as the following: "I feel that this event has become part of my identity" and “I often see connections and similarities between this event and my current relationships with other people” (Berntsen & Rubin, 2006). The CES demonstrates excellent internal consistency with a Cronbach’s alpha score of α=0.94.
Procedure
Participants were asked to provide demographic information, which included age, gender, ethnicity, income, sexuality, and mental health diagnoses (see Tables 1 and 2), before completing the four questionnaires on Qualtrics. The order was the same for all participants (WEMWBS, SCIM, GASP, then CES). Upon completion of the questionnaire, all participants were provided with a debrief sheet which included further information on the study and links to support their own wellbeing.
Power, calculated using G*Power (Faul et al., 2009), indicated that a sample size of seventy-seven participants was required to meet statistical significance and avoid type I or type II error.
Parametric assumptions and scatterplots were calculated in SPSS to evaluate data distribution and check for normal distribution. Then Pearson bivariate correlation and multiple regression analysis were completed before the data were input into Jamovi, where a further Pearson bivariate correlation analysis and two hierarchical multiple regression analyses were completed. These aimed to explore the interaction between centrality of event, wellbeing, shame, and identity.
RESULTS
Notes:
-
Percentages may not total exactly 100% due to rounding.
-
The “Specific Diagnoses” section refers only to participants who self-reported having a diagnosis.
-
The total number of participants is 79 for all categories
The Relationship between Wellbeing and Identity
Parametric assumptions were initially tested, with skew and kurtosis found to be within the thresholds for medium-sized samples (H. Y. Kim, 2013). Since all scores are within the acceptable range, the data are presumed to be normally distributed (Table 3).
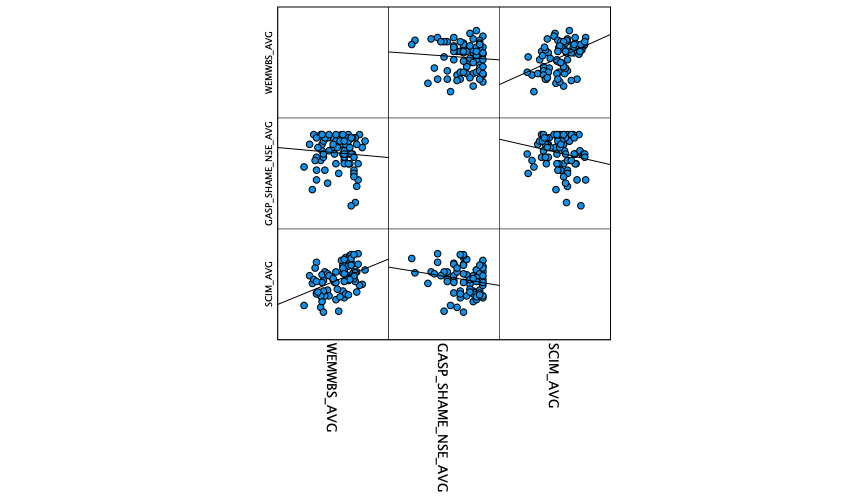
A scatterplot demonstrated the potential for a couple of moderate outliers in the measures (Figure 1). However, these do not appear to be extreme, and after running a box plot analysis, these were not deemed to be problematic. On first inspection, therefore, there is a positive relationship between wellbeing and identity.
A Pearson bivariate correlation was used to explore the relationships between wellbeing and shame, and wellbeing and identity. This showed a significant positive correlation between wellbeing and identity, while no significant relationship was shown between wellbeing and shame (Table 4).
To explore these relationships further, a multiple regression analysis was performed. Identity and shame were entered as the predictor variables, and wellbeing as the outcome. All collinearity results were close to 1.0, indicating no problems with multicollinearity. Again, identity was the significant predictor of wellbeing, with this model statistically significant (R2 = .19, F(2,73) = 8.271, p = 0.001) (Table 5).
The Role of Centrality of Traumatic Event
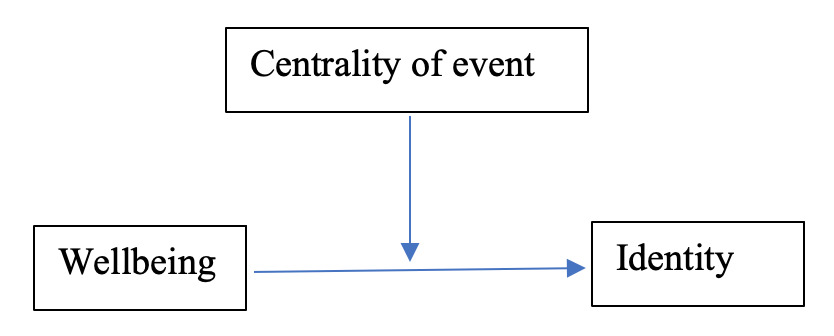
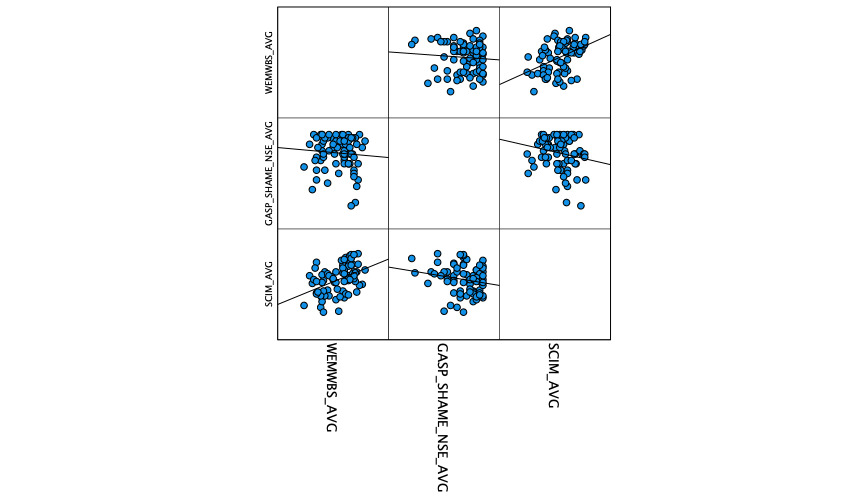
To explore whether the centrality of an experienced traumatic event strengthened the relationship between wellbeing and identity, and wellbeing and shame, two separate moderation analyses were performed. A Pearson bivariate correlation was used to explore the relationships among wellbeing, shame, and identity, with the interaction factor centrality of the event included (Figure 2).
Two significant correlations were found between centrality of event and wellbeing, and centrality of event and identity. No significant relationship was found between centrality of event and shame (Table 6).
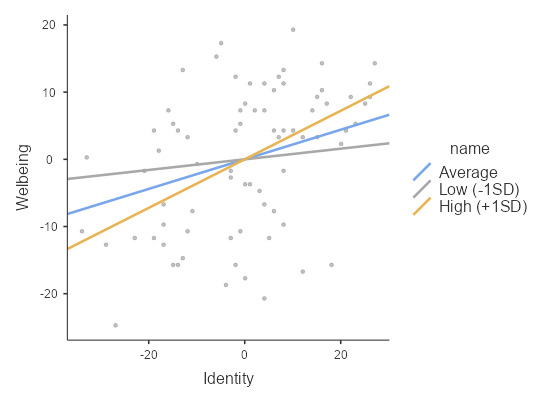
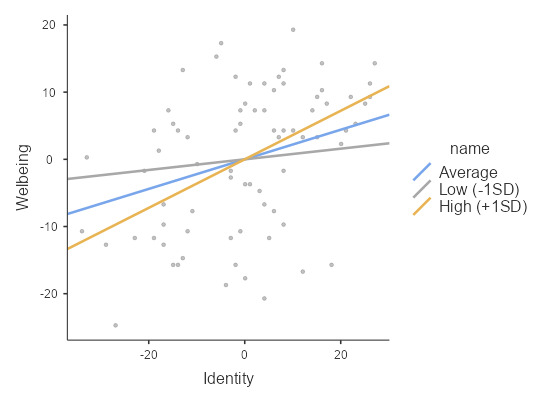
To assess if the association between identity and wellbeing depends on centrality of event (Figure 2), a moderation analysis was carried out. The two predictors and the interaction were entered into a simultaneous regression model. All the collinearity statistics were close to 1, indicating no problems with multicollinearity. The results indicated that trauma (B = -0.18, SE = 0.06, p<.01) and identity (B = 0.22, SE = 0.07, p<.01) both were significantly associated with wellbeing. Indicating that the interaction between identity and trauma was also significant (B = 0.01, SE = 0.00, p<.05), suggesting that the effect of identity on wellbeing depends on the level of trauma. Together, the variables accounted for approximately 26% of the variance in wellbeing, R2 = .259, F(3, 72) = 8.40, p<.001. Further, the simple slope analysis for the association between identity and wellbeing was tested for average (mean), low (-1 SD below the mean) and high (+1 SD above the mean) levels of trauma. Two of the slope tests including average (mean) and High (+1 SD above the mean) indicated a significant association between identity and wellbeing, however, identity was more strongly associated with wellbeing for high levels of trauma (B = 0.36, SE = 0.09, p<.001) than for average (B = 0.22, SE = 0.08, p<.01) level of trauma (Table 7). Figure 3 plots the simple slope for interaction.
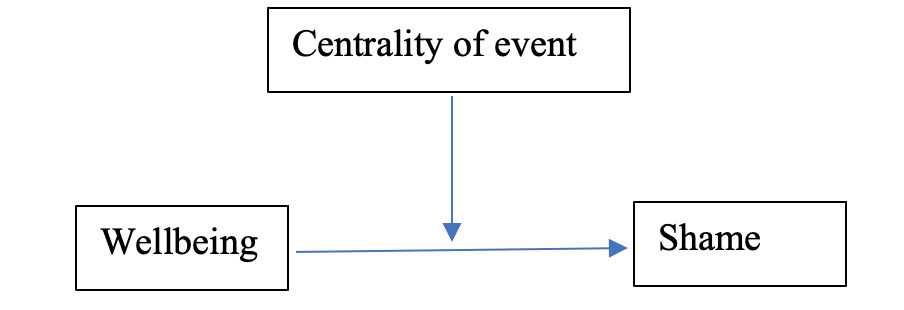
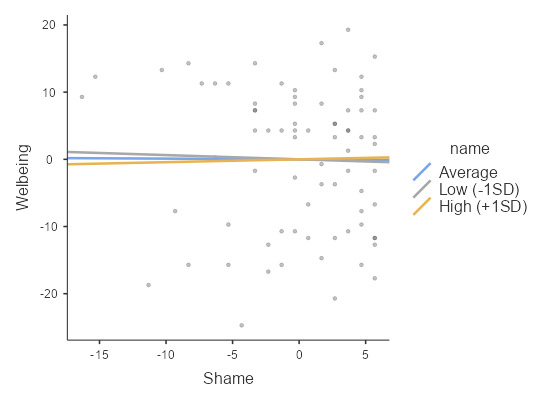
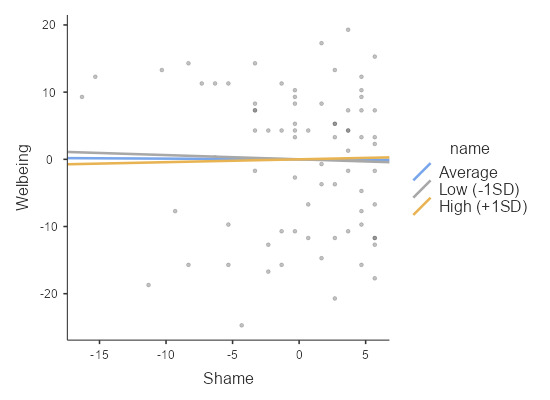
To assess whether the association between shame and wellbeing depends on the centrality of a traumatic event (see figure 4), a moderation analysis was carried out. The two predictors and the interaction were entered into a simultaneous regression model. The results indicated that only trauma (B = -0.20, SE = 0.07, p<.01) was significantly associated with wellbeing. However, the shame and the interaction both were not statistically significant. Table 8 and Figure 5 show detail.
DISCUSSION
The main aim of this study was to explore whether the dependent variables shame and identity were predictors of wellbeing and whether centrality of event strengthened each model/relationship.
The initial findings demonstrated that identity was a moderate predictor of wellbeing. However, there was no relationship found between shame and wellbeing, indicating that shame may not be an effective predictor of wellbeing when considering centrality of a past traumatic event. Many previous studies have found a link between feelings of shame and wellbeing (Rüsch et al., 2013), so this is an interesting finding. The shame-NSE subscale used may not have been suitable to explore the relationship between wellbeing and shame and centrality of event as a moderator of this relationship, due the Shame-NSE subscale measuring an individual’s captures participants’ likelihood of experiencing situational shame in response to hypothetical moral or social transgressions, rather than directly assessing internalized shame around traumatic events that have occurred within their life (Cohen et al., 2011).
Given that the present study also measured centrality of event, the lack of a more trauma-informed or internalized shame measure may have limited the detection of effects. It is possible that shame only significantly predicts wellbeing when it is entangled with core self-concepts, early relational trauma, or persistent negative self-schema.
In contrast, the finding that greater identity disturbance predicts lower wellbeing is consistent with previous research. Sharma and Chandiramani (2021) found a significant relationship between wellbeing and identity status, and these results build upon this. In the present study, identity was analyzed using the overall SCIM composite score rather than the individual SCIM subdomains. This finding also aligns with coaching psychology and positive psychology frameworks, which emphasize the role of self-concept clarity, narrative integration, and strengths-based identity processes in promoting wellbeing and resilience. Although the regression model was statistically significant, the R² value of .19 indicates that a substantial proportion of variance in wellbeing remains unexplained. This suggests that wellbeing is likely influenced by a broader range of psychological and contextual factors beyond identity and shame. Previous research has highlighted the importance of variables such as social support, coping strategies, resilience, and self-esteem in predicting wellbeing. Future research may therefore benefit from incorporating additional predictors to better capture the multifaceted nature of adult wellbeing.
Individuals over the age of 25 may have more developed or stabilized identity structures compared to adolescents, potentially influencing the strength or expression of this relationship. Given that Sharma and Chandiramani’s (2021) original work focused on adolescents, the present findings offer a valuable perspective on how identity coherence continues to play a role in adult wellbeing, particularly during periods of transition or self-reflection.
Conceptually, grounding this research in PERMA+4 positions the study to examine how internal experiences of identity and shame, alongside external environmental disruptions such as trauma, interact with wellbeing in a more complete and contextualized way. In doing so, the study moves beyond deficit-based models of adult mental health, contributing instead to a strengths-informed understanding of what enables people to recover, rebuild, and maintain a sense of wellbeing throughout adulthood.
To measure wellbeing, this study used the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS), a validated 14-item scale designed to capture positive mental health across hedonic and eudaimonic dimensions (Tennant et al., 2007). The WEMWBS has been widely adopted in UK public health research and policy due to its relevance, psychometric robustness, and ease of use with community-based adult populations. While the scale does not map directly onto all nine PERMA+4 domains, it aligns closely with the core principles of positive psychology. It captures an overarching sense of psychological wellbeing that is socially and emotionally grounded. The WEMWBS was developed to assess positive mental wellbeing, incorporating both psychological (eudaimonic) and subjective (hedonic) components (Tennant et al., 2007). While its primary emphasis is on psychological functioning and self-realization, it also captures affective aspects of wellbeing, making it a holistic and strengths-based measure well-suited to adult community populations.
Regarding hypothesis two, and whether centrality of event moderates the relationship between wellbeing and identity, the current model was consistent with the hypothesis that CES will strengthen the relationship between wellbeing and identity. Furthermore, exploration of the simple slopes indicated that the association between identity and wellbeing was stronger at higher levels of CES. Higher SCIM scores indicate greater identity disturbance and lower wellbeing. This relationship was significantly predicted by individuals’ exposure to a traumatic event (CES), particularly when the event had become an integral, negatively defining part of their life story, further strengthening the association. This finding is consistent with previous findings from Merrill et al. (2015) that identity and wellbeing are influenced by an individual’s life story.
For hypothesis three, the current model indicated no association among CES, wellbeing, and shame, a pattern consistent across the simple slope analyses at low, average, and high levels of CES. Therefore, within this model, centrality of event did not strengthen the model between feelings of shame and wellbeing. This correlates with the initial findings, which found no relationship between shame and wellbeing. These findings may add new insight into the impact of centrality of event on internalized shame and wellbeing, for example, previous studies have found that shame was significantly associated with lower wellbeing (S. Kim et al., 2011). However, the population for this study differs from the majority in their meta-analysis, both in age, and as most participants have not been diagnosed with a mental health disorder. This distinction is significant, as this study provides new insight into how centrality of event influences both wellbeing and shame relationships in older, non-clinical populations that coaches are more likely to be working with. Nevertheless, further research is required to explore the broader applicability of these findings to coaching.
The results demonstrating that centrality of event strengthens the relationship between wellbeing and identity is significant. It not only builds upon existing findings but also extends knowledge to a specific age group (over twenty-fives) who are frequently overlooked in identity-related research, as identity consolidation is often assumed to be complete by this stage (Cramer, 2004). This study therefore suggests that identity remains a dynamic and influential construct across the lifespan, with implications for how wellbeing is shaped by the meaning individuals ascribe to life events. This has particular practical relevance for both community mental health workers and coaches working with clients, influencing interventions designed to improve psychological resilience to include those that focus on identity development and coherence. For example, these may consist of integrating narrative approaches, identity mapping, and strengths-based interventions to help participants incorporate central life events into coherent, empowering self-concepts. Approaches could include guided narrative reframing, autobiographical writing, or identity-focused group programs, all of which align with post-traumatic growth and positive psychology principles.
Furthermore, the study’s findings may provide psychologists and coaches with a rationale for broadening the scope of intervention. For instance, interventions could integrate identity-mapping exercises within cognitive-behavioral frameworks or employ positive psychology methods, such as strengths-based identity exploration, to help adults connect personal values with lived experiences. By aligning clinical and community-based practice with the recognition that identity formation and reconstruction remain relevant throughout adulthood, psychologists can better tailor interventions to the nuanced needs of diverse age groups. This would contribute not only to individual wellbeing but also to wider community resilience, reducing the strain on statutory mental health services through more proactive, identity-informed approaches.
Limitations
With only 76 participants, the study was just below the required minimum of 79; therefore, it did not meet the power requirement to sufficiently answer the research questions (Case & Ambrosius, 2007). It is further limited by its focus on the UK only, with a large proportion of participants being white and well-educated. Different socio-economic groups may show slightly different correlations.
It should also be considered that there may be a level of reporting bias in the participants’ answers, as the questionnaires were self-report measures. Therefore, the participants may have altered their answers unintentionally to appease the researcher (Carter et al., 2019). Furthermore, true causal relationships cannot be inferred from the research, as external variables may still have influenced the relationships and results.
Future Directions
The findings of this study point to several meaningful avenues for future research. Most notably, the non-significant relationship found between shame and wellbeing, despite the existing literature suggesting otherwise. This raises important questions about how shame is operationalized, particularly in adult populations. This study represents a critical step in evaluating the limitations of widely used shame measures when applied to adults reflecting on identity-disrupting experiences. The Shame-NSE subscale of the GASP, while psychometrically sound, may not capture the chronic, internalized, or trauma-related shame that is more likely to influence adult wellbeing, especially in contexts where identity coherence and narrative disruption are central.
Future research would benefit from exploring alternative shame measures that are more explicitly designed to assess internalized or developmental shame (e.g., the Internalized Shame Scale [ISS] or the Experience of Shame Scale [ESS]). This would allow for a more nuanced understanding of how shame contributes to adult wellbeing, particularly when it stems from adverse life events perceived as central to the self. The findings suggest that researchers should exercise caution when applying scenario-based shame measures to populations where internalized or trauma-related shame may be more relevant.
In relation to hypothesis two, qualitative data would enable a deeper understanding of how centrality events strengthen the relationship between wellbeing and identity, identifying key themes and providing more detailed data for government bodies to create specific identity interventions and support, as suggested by Baker (2021), to improve the effectiveness of the current approach. These insights carry significant implications for practice and policy. As Baker (2021) notes, existing approaches to mental health provision in England often focus narrowly on symptom reduction, with less attention to identity processes that underpin resilience and long-term wellbeing. By evidencing how centrality of event shapes the identity–wellbeing relationship, such research can inform more tailored interventions that support individuals in integrating significant life experiences into coherent and empowering identity narratives. Additionally, longitudinal or mixed-methods studies could offer insight into how identity, shame, and wellbeing interact over time, especially in the midst of critical life events and previous trauma.
Finally, further research should continue to test the moderating role of centrality of event, particularly in relation to identity and wellbeing. Understanding whether and how event centrality amplifies or buffers the emotional impact of shame may provide greater insight into post-traumatic growth, self-concept repair, and psychological resilience in adulthood. Mixed-methods approaches, combining quantitative and qualitative data, would allow future research to uncover key mechanisms through which CES influences identity and wellbeing, and could inform more targeted, evidence-based policy and practice (Baker, 2021).
CONCLUSION
In conclusion, identity is a significant predictor of wellbeing in adults over 25, and the centrality of experienced traumatic events strengthens this relationship. These findings underscore the importance of integrating identity-focused, strengths-based interventions into community, coaching psychology, positive psychology and clinical practice to support adult wellbeing. Moving beyond symptom-reduction interventions to preventive interventions that actively cultivate identity coherence, strengths, and self-concept integration may support broader community resilience and reduce reliance on reactive mental health services. Future research using mixed methods could further explore the mechanisms by which central life events influence identity and wellbeing, informing evidence-based coaching and positive psychology interventions, theory and frameworks.
AUTHORS

Lauren Barratt is the founder and director of Wellbeing Workshops Devon CIC, a community interest organization delivering evidence-based coaching psychology and psychological interventions across the UK. She is a qualified teacher and psychoeducational facilitator specializing in positive psychology, coaching psychology, and neuroplasticity. Lauren is a member of the BPS with GBC, and has applied for recognition as a Chartered Coaching Psychologist. Her work focuses on delivering trauma-sensitive, strengths-based programmes that translate psychological theory into accessible wellbeing education for underserved communities, addressing health inequalities.

Petra Walker is a Chartered Coaching Psychologist and is the founder of Petra Walker Coaching & Supervision, which offers positive psychology coaching, leadership coaching and coach supervision. She is an author, EMCC Senior Practitioner and holds PCC accreditation with the ICF. She is the Program and Quality Coordinator with the Institute of Positive Psychology Coaching (IPPC).