



Introduction
Coaching a mentee through an issue or challenge, rather than simply telling them how to solve it, can itself be a powerful change- for both mentor and mentee. It can create a dynamic partnership rather than a hierarchy, and it can give mentees both experience and confidence in solving problems for themselves. It also takes the pressure off the mentor, who no longer has to figure out the solution to every problem. – Wisdom, 2025, pp. 95–96
As articulated in the quote above, a traditional mentorship relationship often involves a mentor telling the mentee what to do, based on the mentor’s own experiences and priorities. In contrast, strengths-based coaching centers the learner’s experiences in a shoulder-to-shoulder partnership in which the coachee (i.e., the person receiving coaching) drives the conversational agenda (Boyatzis et al., 2019). Neither top-down nor overtly instructive, the coach utilizes positive regard, deep listening, and thoughtful inquiry to unleash the “coachee’s” innate capacity for evolution, self-direction, and growth.
In such an arrangement, the coachee is encouraged to name a current challenge, explore their own desired resolution, and commit to action in the service of this hoped-for change. Emphasis is placed on the coachee thinking, feeling, and dreaming big to articulate a hoped-for or ideal state that they do not yet have but would love to occupy. It is only then that the conversation moves to action, with the coach supporting the coachee in naming specific steps they could take, evaluate, and celebrate in the service of reaching their ideal.
In academic medicine, data indicate that physicians and trainees who receive this type of supportive, positive psychology-inflected coaching fare better professionally. Specifically, one year into a coaching program, residents at Harvard Medical School reported reduced emotional exhaustion and burnout (Palamara et al., 2015); three years in, ongoing participation, marked by high-quality communication with one’s coach, was positively correlated with enhanced self-confidence, work relationships, and coping with stress (Palamara et al., 2018). Anecdotally, training psychiatry fellows in supportive, compassionate coaching skills that they then integrate into their peer supervision of one another has also been very well received (Boyatzis et al., 2019). Similarly, faculty who receive coaching report enhanced work engagement and decreased interpersonal disengagement (Kiser et al., 2024); physicians across various specialties have likewise exhibited decreased burnout, enhanced quality of life, and bolstered resilience (Dyrbye et al., 2019).
Importantly, in several of the studies described above (Boyatzis et al., 2019; Kiser et al., 2024; Palamara et al., 2015, 2018), coaching was not provided by an extensively trained professional coach brought in from outside the institution; rather, it was faculty with foundational training in the fundamentals of the coaching approach who shepherded these conversations with their mentees and peers. The length of coaching training varies widely across studies, but as few as two hours of instruction for faculty on positive psychology principles and the differences between mentorship and coaching have been associated with positive coachee outcomes (Palamara et al., 2015).
Further, academic medical faculty who have participated in coaching skills training programs report personal gains. These include a greater grasp of the utility and practice of coaching skills, a deeper sense of fostering their own and others’ growth and development (Mukherjee et al., 2024), and reductions in their own levels of emotional exhaustion (Kakarala et al., 2018). An enhanced sense of connection with students, coupled with a deeper appreciation for helping trainees develop more holistically, has also been noted, along with the importance to faculty coaches of ongoing supports and opportunities to debrief together (Brooks et al., 2020).
The promise of such internally created and sustained coaching arrangements is strong for academic medicine. At the same time, the field is not yet fully mature. There is currently limited standardization of quality, consistency, and cost across these various training programs (Bailey et al., 2025)- a gap that is particularly pertinent now, at a time when the coach approach could prove vital in addressing sky-rocketing rates of clinician burnout (Banerjee et al., 2023; Wisniewska & Holt, 2023) and the stresses of research career uncertainty (Pololi et al., 2023). To address this gap and bolster the potential of our faculty, we created the α -LEAP Coaching Skills Training Program (α-LEAP CSP), an in-house coaching skills training program whose cost-effectiveness, curricular standards, and dissemination we could ensure.
In the following pages, we detail the development, delivery, and pilot evaluation of the α-LEAP CSP, which aims to teach early- and mid-career faculty members the fundamental mindsets and skills of the coaching approach within academic medicine. We hypothesize that α-LEAP CSP will demonstrate utility, as evidenced by strong reception among participating faculty and improvements in their self-described professional agency, engagement, and interest in their work.
METHODOLOGY
Development of the α-LEAP CSP
The α-LEAP Coaching Skills Program (CSP) was developed by the first author, a clinical psychologist and faculty member at our institution. For this endeavour, she drew on extensive experience coaching faculty and trainees in academic medicine; coaching coursework that deepened her familiarity with positive psychology and core coaching competencies, and certification as a Professional Certified Coach (PCC) with the International Coaching Federation (ICF). The second and third authors of this manuscript also provided consultation on program development, based in part on joint work co-leading a series of earlier experimental peer coaching groups within our department.
The aim of these earlier groups was to gauge early-career faculty and postdocs’ desire for coaching skills and, anecdotally, to determine how useful participants found these skills for supporting one another and navigating early-career stressors within the academic medical context. Based on the positive responses to this modality, the authors proceeded in the fall of 2024 to build the α-LEAP CSP.
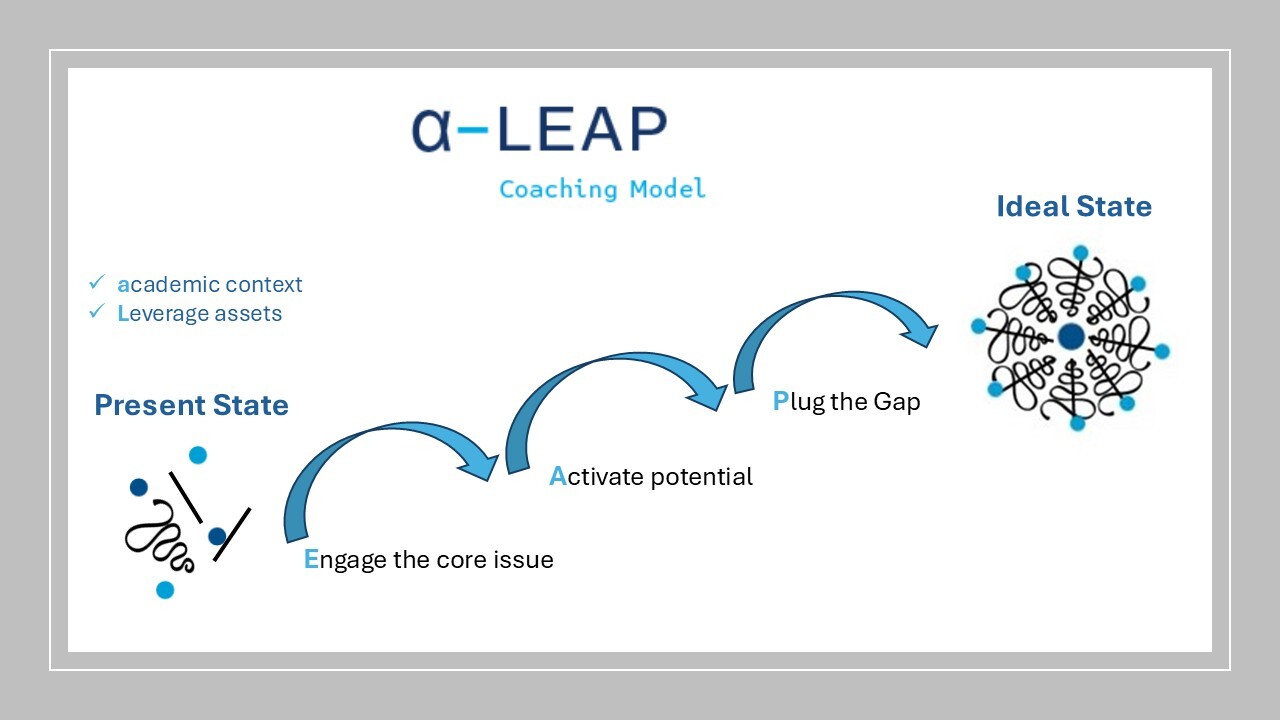
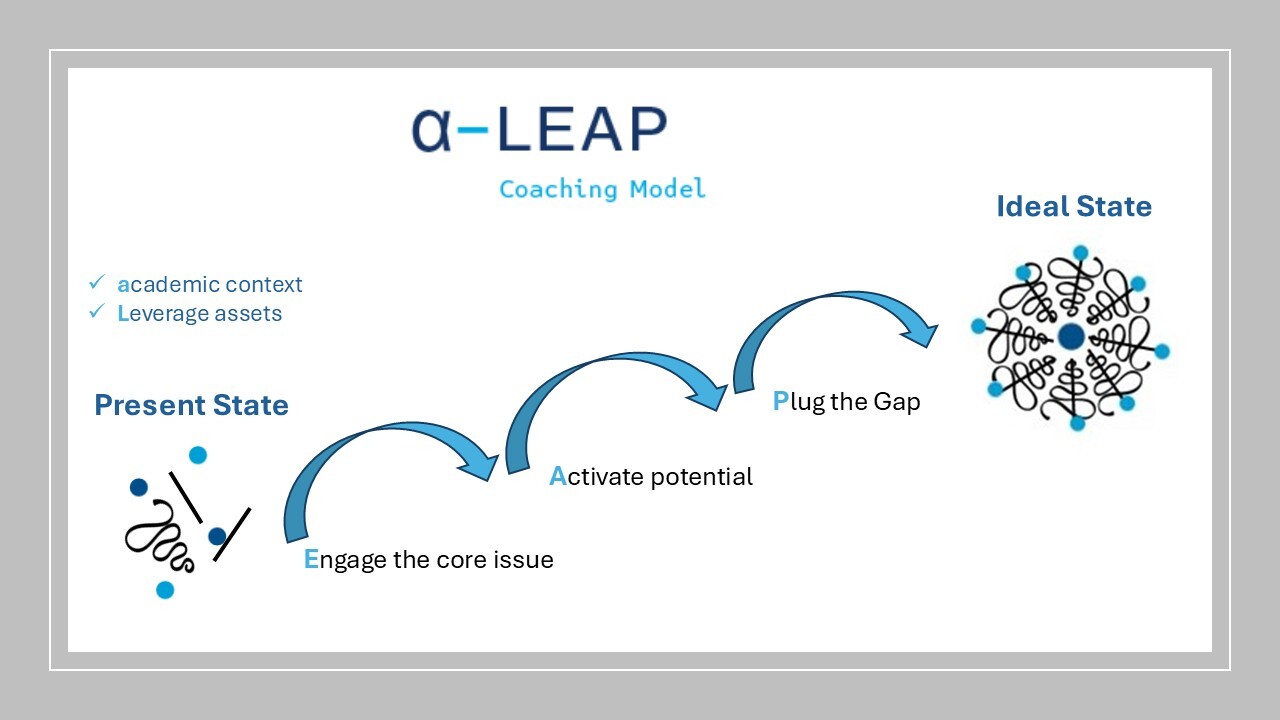
Rooted in strong attunement, positive regard, and following the coachee’s lead, the α-LEAP coaching model aligns with several of the International Coaching Federation (ICF) core competencies (ICF, n.d.). At the same time, the model invites coaches to pay particular attention to the academic medical context in which both dyad members work. This emphasis is consistent with findings from Passarelli et al. (2024), which assert that coaching practices adopted for physicians should be sensitive to the unique stressors these individuals face. Such practices include coaching in line with established principles of positive psychology and behaviour change; remaining aware of the unique challenges and rewards of working within the healthcare hierarchy; and bringing heightened awareness to perfectionism, fear of failure, well-being, and burnout. In the academic medical milieu, we also posit that the coach’s awareness of the stressors inherent to a “soft money” context, stressors exacerbated at the present moment by an insecure grant-funding climate (Tollefson et al., 2025), also matters.
As illustrated in Figure 1, the α-LEAP acronym captures the program’s various emphases, making explicit the mindsets of awareness of academic context and the importance of leveraging personal assets. Likewise, the coach is taught how to utilize positive-psychology-based skills to support the coachee in engaging their core issue, activating potential and possible solutions, and plugging the gap by demarcating their own concrete steps to be taken in service of the desired (ideal) state.
Delivery of the a-LEAP CSP
In the spring of 2025, early and mid-career faculty members from three departments within our school of medicine were invited to participate in the α-LEAP CSP. Departments were chosen based on the interest of their leadership in partnering with this pilot implementation. An advertisement describing the program was shared with these departments to disseminate to their faculty.
The α-LEAP CSP was delivered separately by the first author in each department across three 2-hour group sessions, for a total of 6 hours of training per department; the second and third authors provided support in delivery within our home department. As captured in Table 1, the training consisted of didactics and experiential exercises designed to teach fundamental listening and inquiry techniques, interpersonal stances, and optimal situations for holding effective coaching conversations within the α-LEAP framework. Training sessions were conducted in person and/or over Zoom (varied by department). When appropriate, breakfast or lunch was served.
Evaluation of the α-LEAP CSP
Study Design. The aim of this research evaluation was to gain a preliminary understanding of the impact of the α-LEAP CSP on faculty members’ sense of belonging, well-being, and adjustment at our institution, as well as their understanding and confidence in utilizing coaching skills before and after participation. To track changes over time, the study adopted a longitudinal design, with participants completing pre-program, post-program, and 6-month follow-up questionnaires. This study was deemed exempt by the Yale University School of Medicine Institutional Review Board.
Participant recruitment and consent. Prior to the first session of the α-LEAP CSP, all program participants received an email inviting them to participate in the research evaluation as well. Interested participants were asked to follow an electronic link to the consent form, which stated that data in the form of self-report surveys would be collected pre-, post-, and at 6 months following completion of the α-LEAP CSP. Importantly, all individuals were informed that they would not face any barriers to participating in the α-LEAP CSP training or to their career progression if they chose not to participate in this research study. After reviewing the information, each prospective study participant was asked to provide consent or decline.
The consent process and data collection were conducted through REDCap, an institutional data management system, and were overseen by a research assistant not involved in the α-LEAP CSP program delivery. Only this research assistant had access to information linking participant data to email addresses, which were required to send the consent form and questionnaires to study participants at each time point. Other than these email addresses, no personal identifying information was collected. Further, the researchers analyzing the survey responses had access only to deidentified data, which was no longer linked to participants’ email addresses.
Data collection. Survey data regarding participants’ impressions of the α-LEAP CSP and their sense of adjustment and well-being at our institution were collected at the pre-, post-, and 6-month follow-up time periods. All data collected were obtained through self-report questions developed primarily by the researchers.
These scales were named “Demographics”, “Coaching Skills and Academic Medicine” (23 quantitative items), and “Post-Program Questionnaire” (9 quantitative items, 5 qualitative items). The pre-program assessment utilized the “Demographics” questionnaire and the “Coaching Skills and Academic Medicine” scale, which tapped participants’ knowledge of coaching skills and their sense of adjustment and well-being at our school of medicine. The post- and 6-month follow-up evaluations contained the “Coaching Skills and Academic Medicine” scales, as well as a set of unique quantitative and qualitative items focused specifically on participants’ impressions of the coach approach following engagement with the α-LEAP CSP training (i.e., the “Post-Program Questionnaire”).
All non-demographic, quantitative questions were Likert-scaled from 1 to 5, with 1=strongly disagree/not at all; 4=strongly agree/very much; and 5= not applicable. To avoid inflating the means, any scores of “5” were dropped from the analyses.
Data analysis. Descriptive statistics, including means, minimum/maximum values, and standard deviations, were explored for these data using Excel and STATA/BE v19 (StataCorp). Qualitative data were reviewed for overarching topics and themes.
RESULTS
Demographics. A total of 59 individuals across three departments (Emergency Medicine, the Child Study Center, and Pediatrics) were identified as eligible to participate in the α-LEAP CSP training. Emergency Medicine invited 39 faculty members to join the study; of these, 9-10 individuals attended each of the three α-LEAP CSP training sessions. Participants from the Child Study Center and Pediatrics had received an email about the program and completed a survey expressing interest. Of the 12 who completed this survey in the Child Study Center, 6-10 individuals attended each training session. Of the 8 who expressed interest in Pediatrics, 6-8 individuals attended each training session. Because the program was completely voluntary, attendance by person was not recorded; anecdotally, however, the Child Study Center and Pediatrics hosted the most repeat participants, whereas Emergency Medicine had the most participant variability across the three training sessions.
Across these α-LEAP CSP participants, 9 consented to take part in the study. Table 2 captures the salient demographic variables of this study sample.
Demographics highlight a predominantly Caucasian (n= 9), female (n= 8), clinically-focused (n=9), and early-career (n=6) sample with limited prior exposure to coaching, as either a coachee or person learning about this modality. Most participants (n=7) attended all three of the α-LEAP CSP training sessions, with the remaining two attending two of the three sessions provided to their department. At the 6-month follow-up, 5 of the 9 individuals completed the measures. All of these respondents were female; 3 of the 5 were early-career; and 2 were from the Child Study Center and 3 from Pediatrics.
Self-reported outcomes. Table 3 captures participants’ self-report outcomes associated with the α-LEAP CSP training. Included here is a list of questions designed to gauge participants’ grasp of coaching skills and sense of adjustment at our institution. Pre-, post-, and 6-month follow-up means, maximum and minimum scores, and standard deviations are also included in the table.
Overall, the data reflect the acquisition and retention of coaching skills over time. This is shown in the increase in group mean scores from the pre-training to post-training on items including Question 2 (“In conversation, I know how to invite and validate the viewpoints, hopes, and dreams of those I mentor/supervise”); Question 11 (“I feel confident guiding others to define their own professional paths and aspirations”); Question 12 (“I enjoy taking a strengths-based perspective when helping others”); and Question 19 (“I am confident engaging in a coaching conversation.”). Importantly, at the 6-month follow-up, these means remain elevated over baseline and are, in some cases, equal to or higher than the post-program means.
In tandem, there is a decrease in mean score from pre- to post-assessment on negatively-worded Question 4 (“I do not feel I am a good listener”) and Question 9 (“I do not understand the difference between mentorship, sponsorship, and coaching.”). Similar decreases are maintained at the 6-month follow-up. Taken as a composite whole, these emerging patterns suggest that participants gained and retained a comfort with fundamental coaching mindsets and skills from the α-LEAP CSP training.
A second line of data suggests enhanced professional confidence and values alignment following the α-LEAP CSP. This is illustrated by post-training increases in group mean scores on Question 3 (“I feel confident bringing my values into my professional decision-making”) and Question 5 (“I believe our organizational culture promotes taking responsibility for mistakes”), coupled with decreases on Question 13 (“I am likely to leave my job in the next year”); Question 14 (“I believe our organizational culture punishes people for showing vulnerability and uncertainty”); and Question 21 ("I do not feel confident taking responsibility for leadership challenges within my purview").
Aspects of this hold steady at the 6-month follow-up, with participants reporting their most pronounced confidence in taking responsibility for leadership challenges and an ongoing sense that our organization promotes taking responsibility for mistakes. At the same time, mean responses at 6 months basically return to baseline levels regarding the likelihood of leaving one’s job or perceiving that the organization punishes people for showing vulnerability/uncertainty. Small sample sizes, similar minimum/maximum responses across time points, and relatively large standard deviations make interpretation of these data challenging.
Curiously, immediately following the program, participants noted slightly decreased confidence in coaching skills such as displaying empathy (Question 8) and curiosity (Question 15), as well as increased awareness of rushing to solve others’ problems when mentoring them (Question 20). While we expected these mean values to increase from pre- to post-assessment, we interpret these results as reflecting participants’ growing awareness of the sophisticated nuances and challenges involved in attentive listening, deep engagement with the coachee’s concerns, and resisting the temptation to provide advice. Interestingly, all of these values did follow hypothesized directions at the 6-month follow-up, with individuals feeling more confident than baseline in their capacity to display empathy, remain curious, and not rush into problem-solving mode when helping others. This suggests that an initial questioning of ability due to heightened post-program awareness was later softened and replaced by confidence born of real-time coaching practice.
As revealed Table 4, every item of the “Post-Program Questionnaire” that focused on possible negative side effects of learning the coach approach (such as slowing down one’s work, increasing conflicts of interest or dual roles with colleagues, feeling like an ineffective mentor, or engaging in stilted conversations) was rated very low (means between 1.00 and 1.25, with ranges from “1 = not at all” to “2 = a little”). In contrast, participants voiced particular awareness of how the coach’s approach may have improved their engagement with others at work (mean = 2.78, SD = .44) and helped to decrease their feelings of professional burnout and managing ambiguity (mean = 2.44, SD = .53 for both). Similar results hold up at the 6-month follow-up, with particularly notable endorsement of the coach approach’s heightened engagement at work (mean = 3.20, SD = .45) and its contribution to people feeling valued at work (mean = 2.60, SD = .89).
Qualitative responses highlight new skills learned, including “let the mentee be the expert,” "exploring and sitting with the problem," “asking more open-ended questions to get to a coachee’s values,” and “getting to the underlying issue.” Descriptions of enhanced understanding of the coaching process included greater awareness of the academic context, “the differences between coaching and therapy,” and how the coach is not to act as an expert dispensing advice. These various qualitative responses suggest that participants grasp fundamental tenets of the coach approach, such as the coachee setting the agenda, the importance of engaging with the coachee’s core issues (i.e., values), and the centrality of not mistaking coaching for other supportive relationships.
Further, participants seemed to enjoy the facilitator’s approach and effectiveness in teaching the material. One participant noted, “I benefitted the most from practicing the skills as a group with her guidance after she taught the foundations,” while another commented that the facilitator’s style was “super effective and supportive of the process.” As one participant summed up her experience, "This training helped me feel that my personal and professional growth is valued. It also helped me feel more connected to my colleagues." Responses like these suggest a grasp of the generalizability of coaching across professional relationships in the academic medical context, an appreciation of how the material was taught, and the sense that our faculty feel valued by having access to this sort of program.
Regarding the professional relationships in which they might like to use the α-LEAP coaching skills, participants noted their work with trainees, junior colleagues, students, and peers, while also signalling a desire to obtain additional training and practice in coaching skills, such as practicing with peers or attending related conferences.
Importantly, qualitative responses at the 6-month follow-up indicate actualization of these stated intentions. Specifically, three of the 5 people reported using coaching skills on a weekly basis, and one person reported doing so on a monthly basis. These interactions ranged from work with junior faculty and trainees- “encouraging them to solve their own problems [rather] than immediately jumping in to find solutions,”- to more formal mentorship conversations, in which the mentee is likewise encouraged to "come to their own conclusions."
DISCUSSION
"After a coaching conversation, people should feel charged up, excited, and full of purposeful movement toward their dreams. But it isn’t only the people being coached who will feel charged up. Effective coaches, too, will leave the conversations feeling inspired." – Boyatzis et al., 2019, p. 24
As the quote above highlights, effective, compassionate coaching can empower and enliven those who receive it while also benefiting those who provide it. This paper describes our efforts to harvest the gifts of the coach approach for the faculty at our academic medical center.
Specifically, this manuscript articulates the development, delivery, and preliminary evaluation of the α -LEAP Coaching Skills Training Program (α-LEAP CSP), which aims to teach early and mid-career faculty members the fundamental mindsets and skills of the coach approach in academic medicine. As detailed in this paper, the core tenets and practices of the α-LEAP CSP are rooted within positive psychology principles, coaching competencies as identified by the ICF, and precepts that may be particularly salient when coaching physicians and other individuals working in healthcare/academic medicine (Passarelli et al., 2024).
Also presented are pilot pre-, post-, and 6-month follow-up evaluation data indicating the positive reception of the α-LEAP CSP. As indicated in Table 3, a comparison of pre-, post-, and 6-month follow-up results reflects successful acquisition and retention of the coach approach over time, along with hints of faculty-participants’ sense of well-being and capacity to lead at our institution. Such benefits are echoed in the post-program questionnaire (Table 4), with individuals commenting on skill gains and no drawbacks to having learned the coach approach, with results holding steady at the 6-month follow-up as well.
The various outcomes described above are encouraging; at the same time, this pilot study presents several limitations. These include a small, relatively homogeneous sample (n=9, predominantly female, Caucasian, and clinically oriented; n=5 at follow-up) from which it is difficult to draw fully conclusive results. The exclusive use of self-report data, the inability to distinguish results by department and/or mode of program delivery (Zoom or in person), and the potential confounding of facilitator effects with the salience of program material must also be considered. At the same time, we are heartened to see that the learnings seem to prove “sticky” over time, with individuals at the 6-month follow-up reporting ongoing retention of and utilization of coaching skills with trainees and mentees on a fairly frequent basis.
Building on these preliminary findings, our current aspiration is to hone the α-LEAP CSP in such a way that faculty at our and other institutions and others can more easily gain and utilize the skills and mindsets of the coach approach. Given that traditional coach training can be an expensive proposition, our capacity to disseminate the α-LEAP CSP internally, without charge, helps foster adoption of the coach approach across the academy at a time of heightened vulnerability to resource constraints. Further, the promising results of this pilot study have positioned our team to take several steps in line with our larger aspiration, which is to move the culture of academic medicine in a more humanistic and collegial direction that encourages deeper values expression, interdependence, creativity, and resilience on the part of trainees and faculty (see, for instance, David, 2024).
The first step includes continued advertising within our community about the coach approach and the availability of the α-LEAP CSP. New training sessions will be scheduled as requested, once a critical mass of faculty members has expressed interest. Also underway are internal initiatives that would enable formalized scaling of α-LEAP CSP, including offering continuing medical education credits for the training, copyrighting the materials, and building out a website. The possibility of preparing other faculty to facilitate the α-LEAP CSP (i.e., a train-the-trainer model) is also under consideration.
Finally, beginning in the fall of 2025, the first author rolled out α-LEAP WRAP (Wraparound), an expanded version of the α-LEAP CSP that provides faculty with a slightly lengthened version of the CSP training detailed in this manuscript. Based on anecdotal requests from α-LEAP CSP participants for more structured time to practice coaching skills, α-LEAP WRAP expands the standard CSP training to 8 hours of didactics and experiential exercises. Participating faculty who complete the training are also invited to join an ongoing, biweekly “Community of Practice” meeting during which they may discuss their coaching challenges and successes, as well as an annual half-day “α-LEAP Collaborative” retreat where they will receive additional coaching instruction and can network with one another.
A novel, complementary facet of α-LEAP WRAP is a 3-hour orientation for trainees and fellows on the culture of academic medicine, the differences between mentorship and coaching, and the best ways to approach a coaching relationship. The purpose of this training is to set expectations and position fellows and residents to receive coaching optimally. We also hope to obtain a multi-modal perspective on the optimal “dose-response” that allows participants at all professional levels to seize the benefits of learning the coach approach through the program. By targeting fellows and residents to receive coaching and departmental faculty to receive coaching education; by providing ongoing support to these faculty coaches for the duration of the trainee-faculty relationship; and by evaluating standard outcomes, including physician burnout and coachees’ perceptions of their faculty-coach’s effectiveness, α-LEAP WRAP ultimately endeavours to weave a culture of coaching skills training vertically and horizontally through the fabric of our medical school.
While not a panacea for all that ails our faculty, fellows, and residents, building an effective, sustainable, and replicable coaching infrastructure holds promise for unleashing the potential, well-being, and generativity of the academic medical workforce. Ultimately, we hope that the seeds sown by the α-LEAP CSP and its offshoots will sprout many opportunities for the faculty and trainees working across our academic medical ecosystem to flourish more fully and interdependently with one another.
AUTHORS

Daryn H. David, PhD, PCC, is a licensed clinical psychologist, academic, and professional certified coach through the International Coaching Federation. At the Yale School of Medicine, Dr. David is an Assistant Professor at the Child Study Center and serves as Director for Leadership Development and Coaching Initiatives in the Offices of Academic & Professional Development (OAPD) and Collaborative Excellence (OCE). Through dynamic leadership development programming, coaching, and scholarship, she leverages her expertise to help academics and health care providers, including those from traditionally underrepresented backgrounds, actualize their fullest professional potential.
Dr. David holds a Bachelor of Arts (AB) degree in Social Studies from Harvard University and a PhD in psychology from Yale University, where she likewise completed her predoctoral clinical internship and postdoctoral fellowship.

Dr. Victor Avila-Quintero graduated from the School of Medicine at Universidad de Especialidades Espíritu Santo in Guayaquil, Ecuador. He is an Associate Research Scientist at the Yale Child Study Center in Dr. Michael Bloch’s lab. His work focuses on statistical analysis and meta-analysis across projects in general, child and adolescent psychiatry, and addiction psychiatry. He is also committed to creating learning opportunities for mentees in psychopharmacology clinical trials and research methodologies.

Dr. Angeli Landeros-Weisenberger graduated with a degree in medicine from La Salle University in Mexico City, Mexico, and did her training in Psychiatry at the Hospital Español and the Universidad Nacional Autónoma de México (UNAM) in the same city. After graduating, she came to Yale University through the American Psychiatric Association (APA) Minority Training grant (PMRTP) to do her research fellowship under the mentorship of Dr. James F. Leckman at the Yale Child Study Center, focusing on novel evidence-based psychotherapeutic interventions for mental disorders across the lifespan. She has expertise in the assessment of mood disorders, Tourette syndrome, obsessive compulsive disorder, trichotillomania and anxiety disorders, among others. She also has expertise in conducting and implementing clinical trials in these same conditions, both with industry and NIH. She enjoys teaching medical students about these disorders and training them in evidence-based techniques. She currently serves as a Co-chair of the Pediatric Protocol Review Committee (PPRC); is a member of the Yale Human Investigation Committee 4-B; is an elected voting member of the EPCC; and is the SWIM liaison for YCSC. She is a mother of three and is constantly searching for the ever-elusive work-life balance.

Dr. Linda Mayes is the Arnold Gesell Professor of Child Psychiatry, Pediatrics, and Psychology and Chair of the Yale Child Study Center in the Yale School of Medicine. Trained as a pediatrician and child and adult psychoanalyst, Dr. Mayes’ research focuses on early childhood adversity and its impact on socio-emotional and cognitive development from infancy through school age. Taking a two-generation perspective, Dr. Mayes also studies the psychobiological underpinnings of parenting and how conditions such as substance abuse impact the adult transition to parenthood. A theme running throughout Dr. Mayes scholarly work is the central role of human relationships in supporting children’s adaptive development and flourishing as adults. An author of over 350 peer-reviewed papers and 100 review chapters, her work appears in the developmental psychology, pediatric, behavioural neuroscience, and psychoanalytic literature. She is also the author of seven edited books on topics such as parenting and substance abuse, developmental research, and three books for parents and teachers on parenting and fostering resilience. Dr. Mayes is also a visiting professor at Sewanee: The University of the South, where she collaborates on courses on historical trauma, psychological journeys across the lifespan, and child and family development in rural Appalachia.